
Study design
INMA Cohorts
The INMA Project is based on the experience acquired by groups that studied several cohorts with different objectives: the cohort of Riera d’Ebre (n=102), an area with high levels of organochlorine compounds and mercury, evaluated the relationship between these exposures and the neurological development of the children; the cohort of Menorca (n=492), studied the relationship between the early exposure to irritating of the air and allergens with the development of allergy and asthma; and the cohort of Granada (n=668), that studied the incidence of reproductive disorders in men in relation to the exposure to endocrine disruptors.
Based on the experience of these previous cohorts, other 4 new cohorts were designed to evaluate the impact of environmental exposures in children’s health: Valencia (n=787), Sabadell (n=622), Asturias (n=485) and Gipuzkoa (n=612), that followed the same protocol.
INMA Population
The population of the study are pregnant women of the general population who lived in each area of study (Ribera d’ Ebre, Menorca, Granada, Valencia, Sabadell, Asturias, and Gipuzkoa (Figure 1) and their children.

Figure 1. Geographic localization of seven INMA study areas in Spain.
The criteria of inclusion of the mothers were:
- To belong to the study area (specific of each cohort).
- To be minimum 16 years.
- To have a unique pregnancy.
- Not to have followed any program of assisted reproduction.
- To give birth in the reference hospital.
- Not to have communication problems
Each cohort had different periods and types from recruitment. In the cohorts of Ribera d’Ebre and Granada, the mothers were recruited during the admission to the hospital at the moment of the childbirth. In Ribera d’Ebre, the recruitment was between March 1997 and December 1999, whereas in Granada it was between October 2000 and July 2002. In Menorca, all the eligible women who went to the prenatal visit in some of the sanitary centres of the island (private or public) were invited to participate in the study, and the recruitment lasted a year starting in July 1997. In the 4 new cohorts the recruitment took place during the first prenatal visit (between weeks 10 and 13 of gestation) in the public hospital of reference or in the health centre of the area. The periods of recruitment went from February 2004 to June 2005 in Valencia, from July 2004 to July 2006 and May 2007 to July 2007 (there was an additional round of recruitment) in Sabadell, from May 2004 to June 2007 in Asturias, and from April 2006 to January 2008 in Gipuzkoa.
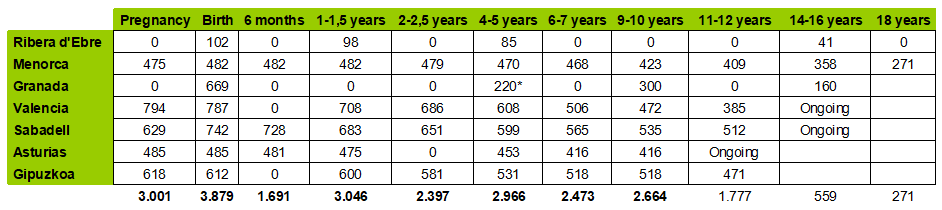
*Subgrup
The study was approved by the Ethical Committee of the Municipal Institute of Medical Investigation and by the Ethical Committee of the hospitals involved in the study. The pregnant women received information of the study both written and orally. Their informed consent of the participants is asked in each of the visits.
Visits
Each cohort has small variations in the visits, although the key ones have been made in all cohorts (pregnancy, childbirth, at age 1 and at age 4). In Ribera d’Ebre and Granada, the visits were made at birth, at age 1 and at age 4. Although the mothers were not followed up during pregnancy, they answered a complete retrospective questionnaire on the pregnancy. In Menorca, the follow up began during pregnancy, and it was continued at childbirth, 3 months, age 1, age 2, age 3, age 4, age 6, age 7.5 and age 10.5. In the 4 new cohorts new, the first visit was during the first trimester of pregnancy and it was repeated in the second and third trimesters, at childbirth, at 6 months (only in Sabadell and Asturias), at the 12-18 months, and at 2-2,5 and 4-5 years. The visits will continue throughout his life if there is enough funding.
Collection of data
The collection of data presents small variations between cohorts as per their internal interests, but the main variables have been gathered in all INMA cohorts. Extensive evaluations to the pregnant women and the children have been made. The information has been taken from several sources: questionnaires (made by trained interviewers), clinical data, physical exploration, biological echographies, samples (blood, placenta, tinkle, saliva, maternal milk, hair and nails), environmental determinants of the diet and measurements (air and water pollution, persistent and semipersistent polluting agents).
